 |
Department of Radiation Oncology |
 |
|
Department of Radiation Oncology |
|
| RETURN TO JOHN SOKOL'S HOME PAGE |
COMBINED INTERSTITIAL IRRADIATION AND HYPERTHERMIA IN THE
TREATMENT OF PROSTATIC CANCER
M.A. Bagshaw, M.D., R. Ben-Yosef, M.D., P. Fessenden, Ph.D.., D.R. Goffinet, M.D., I.D. Kaplan, M.D., D. S. Kapp, Ph.D., M.D., A.W. Lohrbach, J. M. Mariscal, A. N. Peters-Brown, S.D. Prionas, Ph.D., M. C. Smitt, M.D., J. L. Sokol
While external beam radiation therapy is often successful in the treatment of pro-static cancer, the success rate is stage-dependent, decreasing in the more advanced stages 1,2. Also, the incidence of post-treatment positive biopsies increases with advancing stage, and the disease-specific survival is significantly better, stage-for-stage, for patients in whom control of the disease at the primary site is achieved3. One concept which promises the achievement of better local control is to deliver a higher dose of radiation to the primary site. Our present external beam technique delivers 70 Gy in seven weeks to the prostate.
This dose can be increased by using a combination of external beam irradiation which is boosted at the primary site by an interstitial implant. In the system under investigation at Stanford, 50 Gy in five weeks is delivered to the prostate and the pelvic region with external beam irradiation at 6 or 15 MV. A two- to three-week period of rest follows. Then, with the patient anesthetized, 17-gauge template-guided trocars are inserted through the perineal skin into the prostate 4,5. These metallic trocars will contain afterloaded iridium-192 sources, and will be used as conductors of 0.5 MHz radiofrequency current which induces hyperthermia in the prostate. Illustrations of the procedure are shown in figures 1 and 2. By this technique, an additional 30 Cy is administered to the prostate in approximately 40 - 60 hours, and one 45-minute hyperthermia treatment is administered immediately before inserting the iridium-192 afterloading catheters, and again, immediately after their removal. Thus, the patient receives a total radiation dose of 80 Gy, rather than the customary dose of 70 Gy, and, importantly, the 30 Gy administered interstitially is combined with two hyperthermia treatments.


| Case #1: The patient is a 76-year old white male who had a relatively small, but still extracapsular, T3 carcinoma of the prostate. The pretreatment prostate specific antigen (PSA) was 75.4 ng/ml, and there was no evidence of metastases. The interstitial implant was carried out 26 days after the external beam irradiation by the insertion of twelve metallic trocars to carry the iridium-192 and two nylon trocars for longitudinal temperature monitoring. Sixty-eight iridium sources were inserted and remained in place for 54 hours, with a total activity of 42.66 mCi. The temperature distribution for the first hyperthermia treatment is shown in figure 3. | 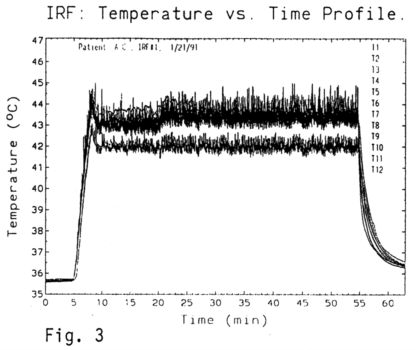 |
|
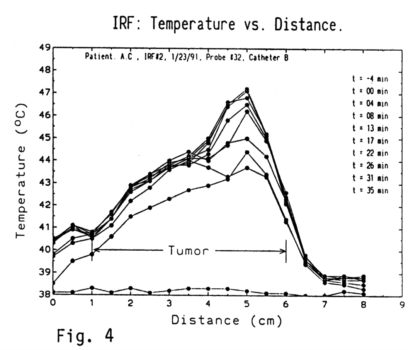
The temperature was monitored at the midpoint of the active section of each trocar with a Bailey thermocouple; the shanks of the trocars were electrically insulated to prevent heating of normal tissue between the perineum and the prostate. A steady state was achieved in about five minutes,and the temperature for ten of the trocars was relatively homogeneous between 43 and 44.5 degrees. Two of the trocars were controlled at a slightly lower temperature (42 degrees) because they were situated directly in the rectal submucosa. Note that after approximately 15 minutes of heating, the power was increased slightly, raising the temperature throughout the implant another one-half of one degree. figure 4 shows the temperature as monitored by a luxtron fiber optic probe which traversed along the length of the nylon catheters, reading the temperature at half-centimeter intervals at different times during the heating process. |
 |
| Figure 5 is a temperature vs. time profile in which the temperature curves are averaged over 60 seconds. | 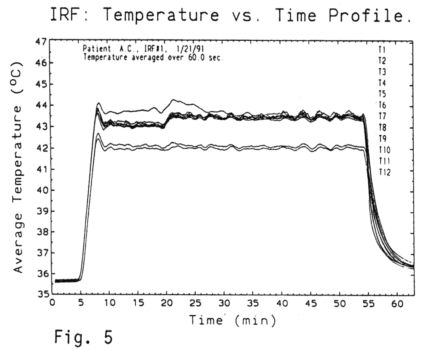 |
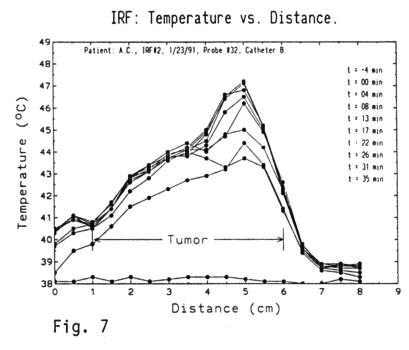
Figures 6 and 7 show the temperature vs time profile and the temperature vs. distance profile for the second heating episode Notice the high degree of concordance between the first and second heating sessions.
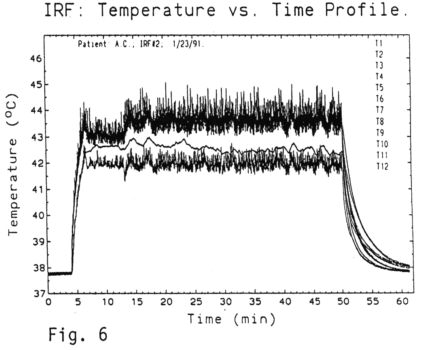
The patient recovered without incident, and at eleven
months is living without evident disease, and with complete resolution
of the tumor on rectal examination. Prior to the therapy, the PSA was 75.4
ng/ml; at two and one-half months it had dropped to 13.1; and at eleven
months to 1.3.
| Case #2: The second patient is a 65-year-old physician who had a 2x3x3 cm T3 nodule at the right base of the prostate, which extended beyond the prostatic capsule. His initial PSA was 21.6 ng/mI, and there was no evidence of metastases. He received 50 Gy external beam, and, after a 13-day intermission, a hyperthermic implant. Thirty-six treatment trocars and two monitor trocars were placed. The treatment trocars were loaded with 148 iridium-192 sources, with a total activity of 137.2 mCi, which delivered 82 cGy/hour for 36.6 hours, to a minimum volume of 80 cc. This is one of the largest implants that we have accomplished, and the resulting temperature vs. time profile is illustrated in figure8. | 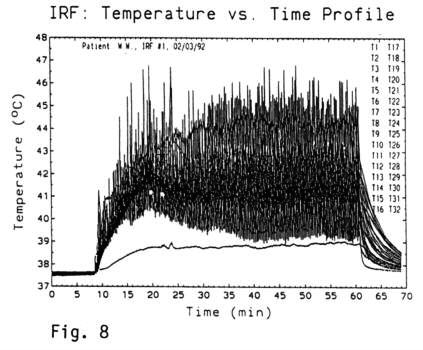 |
| This demonstrates that the temperature distribution reached a steady state of between 40° and 47° C in about six minutes, and was held for 45 minutes. This is perhaps better demonstrated in figure 9, which shows the temperature vs. time profile averaged over 60 second intervals. Inspection of figure 9 demonstrates that most of treatment volume is held between 41° and 42° C, with highs that reach to 44.5° C Figure 10 shows the temperature profile along the length of the catheters at different time intervals. | 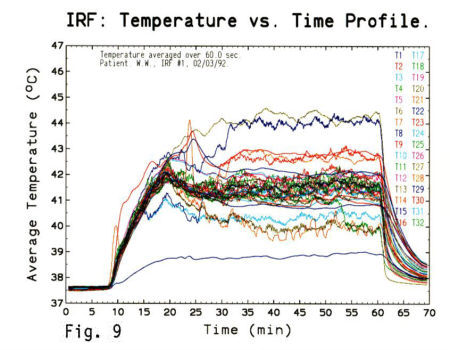 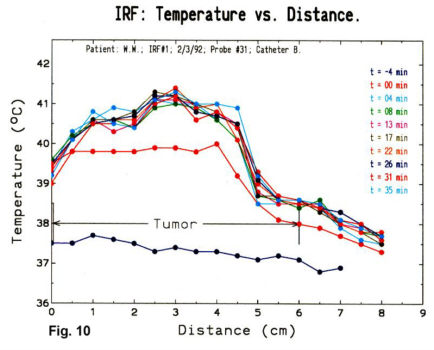 |
| The heating episodes were a trying experience for
this patient even though an epidural drip was in place. The medications
used during the heating were Fentanyl and Ketamine, but a true saddle-block
was not used. At the conclusion of this implant, and upon review of the
previous experience, it was decided that the procedure was too stressful.
Accordingly, in consultation with Anesthesia colleagues, it was decided
to administer true epidural anesthesia during the heating sequence.
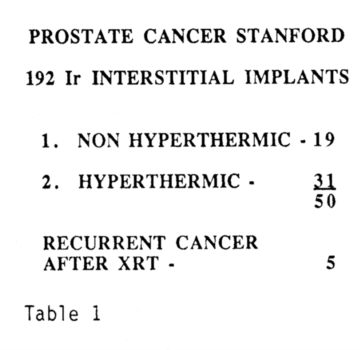
Subsequently, two major changes were introduced. The first was the elimination of the laparotomy and the placement of the trocars percutaneously under transrectal ultrasound control. The second was the introduction of true epidural anesthesia during the heating episodes, and also during the removal of the implanted trocars The epidural catheter is placed prior to the general anesthesia for the implant procedure. Pulse and blood pressure monitors are affixed, and an IV is established. During the heating episodes, 2% lidocaine without epinephrine is administered in the epidural space in two or three 5 ml increments, controlling for perineal sensation with a pin prick. During the period of bed rest (40 - 60 hours) between heat applications, dilaudid is infused into the epidural space at the rate of 0.1 - 0.2 mg/hour. The total implant early experience is summarized in Table 1. This
table does not include the patient who was implanted without a suprapubic
exploration.
|
 |
| In addition to the 31 patients reported here, five other patients were implanted for recurrent disease. These patients are not included further in this series. One patient has failed with metastatic disease, one has apparently failed locally with a positive biopsy, and two patients have had elevations of the PSA. Table 2 demonstrates the PSA response following the iridium-192 hyperthermia implants. In 18 of the 31 patients, the PSA decreased to the normal range. | 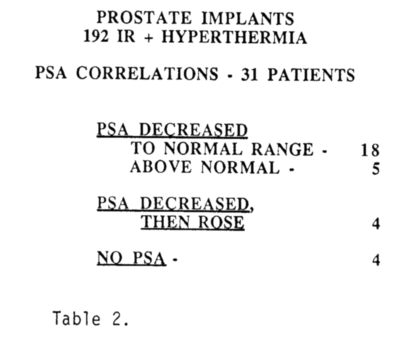 |
Thirteen complications have been encountered. There were two patients with venous thromboses, and one with a pulmonary embolus. A wound infection occurred in two, and a lymphocele in one. Bedsores occurred in two patients, but these healed rapidly and probably represented pressure sores induced by the template. Two patients required temporary catheterization and in one patient this induced a trigone ulcer. An unexpected complication was the induction of penile pain and numbness. This was manifest by a curious combination of loss of sensation and burning discomfort in the glans penis, which was encountered during the heating sessions but which also was persistent in three patients. In two patients the symptomatology is receding; however, in one patient who had an extensive implant, this sequela, although receding, still remains a notable problem nine months after the procedure. There has been a preservation of erectile potency in 50% of the patients treated, which is essentially identical to that seen after external beam irradiation in our series
The complexity of the implants has increased with time and experience. Between 1987 and 1991, an average of 14 trocars per patient were placed; between 1991 and 1992, 26 trocars per patient have been used. While this has been the result perhaps, of patient selection, it also represents an increase in confidence with the procedure. Presently, not enough time has elapsed to demonstrate an increased efficacy either for the addition of the iridium-192 boost, or the iridium-192 boost plus hyperthermia. Thirty-one patients have received triple modality treatment consisting of external beam plus iridium-192 boost, plus hyperthermia, while 19 patients have received external beam plus iridium192 alone. 'This has increased the total radiation dose to the prostate to 8000 rad, i.e., 5000 rad fractionated at 200 rad per day over five weeks by external beam plus 3000 rad interstitial boost in approximately 40 - 60 hours The hyperthermia, while not exactly concomitant, is administered immediately before and then immediately after the placement of iridium. To date, 110 patients have succumbed to prostate cancer. One patient who received a hyperthermic implant died of a heart attack while skiing. Another patient died with advancing cancer, and a third died of cardiovascular disease with a rising PSA.
Four of the patients who have been treated with a hyperthermic implant appear to have relapsed, one with an apparently positive biopsy, one with metastatic disease, two with rising PSA values. Eleven of the 19 patients who received the iridium-192 boost only have relapsed. The difference between the two groups, however, is not significant and the follow-up is too short for the patients who received the hyperthermic implant to be of any consequence.
In summary: External beam irradiation followed by an interstitial boost of iridium-192, which can be energized with radiofrequency current to induce hyperthermia has been developed. This raises the total radiation dose to 5000 rad external beam plus 3000 rad brachytherapy, with two hyperthermia treatments. The technique has evolved from an open surgical procedure to a closed transrectal ultrasound-guided implant. Although there was significant discomfort associated with both the hyperthermia and the removal of the implanted trocars for the patients treated earlier in this series, better utilization of prolonged epidural anesthesia has greatly improved patient tolerance.
This technique clearly permits an increased physical radiation
dose to the prostate for the treatment of carcinoma and perhaps offers
physical enhancement of the biological effect.
1. Bagshaw MA, Cox RS, Ramback JE. Radiation therapy for localized prostate cancer. Urol Cl of No. Amer 1990; 17:787-802.
2. Ray CR, Bagshaw MA, Preiha F. External beam radiation salvage for residual or recurrent local tumor following radical prostatectomy. J Urol: 1984; 132:926-930.
3. Kaplan 1K, Prestidge BR, Bagshaw MA. The importance of local control in the treatment of prostatic cancer. r Urol 1992; 147:917-921.
4. Goffinet DG, Prionas SD, Kapp DS, Samuiski TV, Fessenden P, Hahn
GM, Lohrbach
Aw, Mariscal IM, Bagshaw, MA. Interstitial 192-Ir flexible catheter
radiofrequency
hyperthermia treatments of head and neck and recurrent pelvic carcinomas.
Int
J Radiat
Oncol Biol Phys: 1990; 18:199-210.
5. Bagshaw, MA, Prionas SD, Goffinet DR, Cox RS, Kapp DS, Freiha
F. External beam irradiation combined with the use of 192-iridium implants
and radiofrequency-induced hyperthermia in the treatment of prostatic carcinoma
In: EORTC Genitourinary Group Monograph 10: Urological Oncology: Reconstructive
Surgery. Organ Conservation. and Restoration of Function. Smith PH,
Pavone-Macaluso M, eds. New York: Wiley-Liss, Inc 1991; 276-279.